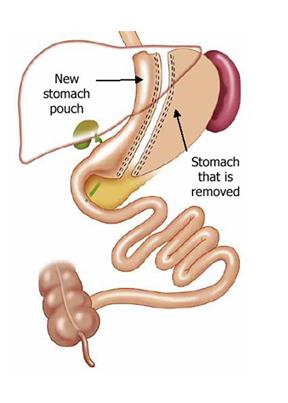
A sleeve gastrectomy is a laparoasopic (keyhole) restrictive surgical proceedure that reduces the stomach capacity thus diminishing the volume of food able to be eaten.
Typically the stomach can hold upto 1.5 L of food stuffs, but this is reduced appoximately 90% to a volume of 150-200mL.
How does it Work
The stomach volume reduction enables only small amounts of food to be eaten, before satiety (feeling of being full) occurs, stopping the desire to eat further. This reduced calorie intake combined with the more rapid transit of food into the small bowel results in weight loss.
Progress
Patients after a sleeve gastrectomy will be on fluids for two weeks then onto a puree diet for two weeks then onto solid food. A two night stay in hospital is expected.
Expected Outcomes
Typically patients will lose weight with the the majority losing 50-70% of their excess weight over 2 years. The initial weight loss is more rapid but slows over time. Weight loss does differ between people.
Risks
All operations have risks, general and specific, this list is not comprehensive but includes the most commonly seen ones.
General risks
• Bleeding
This is uncommon and is treated at the time of surgery. It typically occurs at the new staple line and only very rarely requires a blood transfusion
• Infection
Uncommon, but occassional occurs at the incision sites and may require a course of oral antibiotics
• Pain
Is typically minmal and simple oral analgesia is required but sometimes stronger pain killers are required.
• Damage to surrounding organs
This is unlikely especially at laparoscopic proceedures but damage to the spleen or bowel can occur and this is typically repaired at the time of surgery
• Blood clots (Leg or Lung)
This is rare, and preventative measeures such as stockings, and intra-operative calf compression devices are performed routinely. In addition all patients receive blood thinning injections to reduce the risk of clots forming.
Specific
• Gastric reflux
As the stomach is narrowed down sometimes acid will reflux into the oesophagus, this occurs in upto 10%. Typically this signifcantly reduces/resloves with resolutionof the inflammation following surgery. Occassionally pateint will require anti-acid medication
• Staple line leak
This occurs in 0.5- 1% of patients are is the most serious complication. This occurs at the top of the stomach as it has the poorest blood supply. The leak allows gastric contents into the abdomen causing peritonitis, and can occur upto 14 days after the operation.
• Stenosis
Rarely excessive scarring occurs at the staple line and narrows the new stomach lumen preventing easy passage of fluids and food. This reuires a gastroscopy and dilation to improve the narrowing.
• Sleeve dilation
Overtime if small meal volumes are not adhered too some patients can stretch the stomach so they can eat larger volumes of food. This results in weight regain, twith the only intervention being further surgery.